Quote:
Originally Posted by Lisa V

Lately, however, I keep hearing from people who have relapsed after transplant, and even some of the doctors in the AA&MDSIF's videos refer to relapses post-BMT, and also say that there is no significant difference in the survival statistics between BMT and IST (where that is an option). So for me, that puts the "cure" aspect in a somewhat different light. If relapse is a possibility in both scenarios, and so is durable remission, then it's not so clear cut.
|
Hey Lisa!
I'm glad you brought this up. I noted up front that it's kind of a controversial subject, because it's important to be 150% behind whatever decision you finally make. And STC is a real miracle for some people -- often people who really and truly have no other viable option.
But, when you're making a decision, it's also important to look at all sides of the issue -- and to understand that transplanting a 15-year-old with AA is very, very different than transplanting a 50-something with high-risk MDS. That's why I really really like the
Matt Kalaycio presentation, because he's a transplanter, but he's very, very clear about how risky an option that is. He also talks about STC as "potentially curative," which is a better formulation than saying it's "the only cure for MDS."
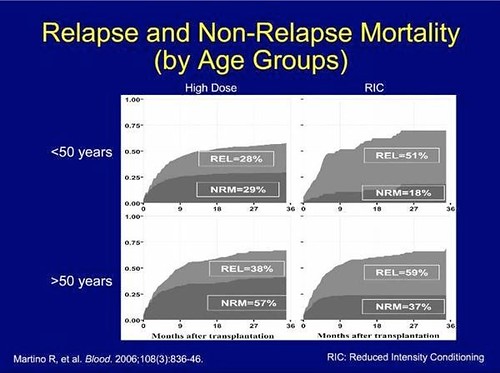
Here's a famous graph that you've probably seen in the presentations or the literature:
 13.SCT Comparison Study
13.SCT Comparison Study by
hankins.greg, on Flickr
So, what does it say? It's comparing "big" myeloablative transplants (on the left) with a reduced intensity "mini" transplant. REL is relapse and NRM is "Non-Relapse Mortality"
So, the graph shows that, after three years, amongst folks under 50 years of age, three years out, there's a 29% chance the transplant will have killed the patient, and a 28% chance they will have relapsed. Among older folks, there's a 57% chance the transplant will kill you and a 38% chance you'll relapse. If you look at "mini" transplants among older folks, the percentages are reversed -- less death, more relapse.
Now, all the usual caveats apply. The study was done in 2006, the data is from 1998-2001. Presumably, transplanters have gotten better in the intervening years. There were all sorts of folks in the sample from really high risk to relatively low-risk. If you're a really healthy 50-something hot dog, you're likely to do a lot better and not be in either the dead or the relapsed category.
Still, amongst the 171 patients over 50 in this sample who had a standard ablative transplant, there was a nearly six in ten chance they'd be dead in ten years -- and a nearly four in ten chance they'd relapse.
These are scary numbers for a therapy that's supposed to be a "cure." If you go and spend a week reading
The Emperor of All Maladies (which I reviewed
here), you'll learn a bit about how "cure" became the key word in cancer research, and how that may have been more about politics and marketing than about medicine.
Many, many, many folks really, really need a transplant. It is truly the very best option for many people. I fully expect that I will have one, and I admire and value the wonderful folks who have shared the good, the bad, and the ugly of their transplant experience on these forums, so we all can learn.
But, when I hear that a doctor has advised transplant for a patient with no clinically significant symptoms, no transfusion requirements, and excellent quality of life, it pretty much curls my hair, after which steam starts shooting out of my ears. I understand that some folks, like Dr. Bart Scott himself, have to be cured at all costs. But, from my perspective as a patient trying hard to be educated about my options, it's not really responsible medicine to lead folks down that road without first being really honest about what they are getting into.
Take care!
Greg