On Day 7 of the NIH Campath trial, the fifth full 10 mg dose of Campath produced the now-expected and somewhat boring result of no chills, shakes, or fever.
The morning's blood draw, however, produced something quite a bit more interesting.
 0001zl copy
0001zl copy by
hankins.greg, on Flickr
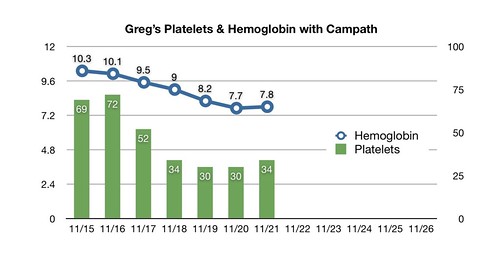
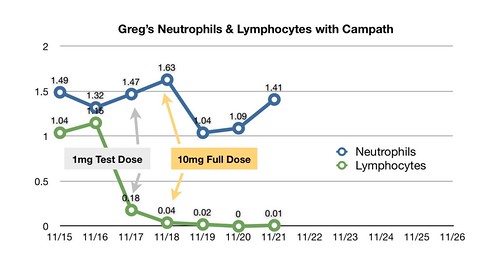
We were scheduled for two RBC transfusions today, based on a CBC from yesterday that showed hemoglobin at 7.7. And we expected this morning's 5:00 am blood draw to produce an Hgb result in the low sevens. Instead, we got a 7.8. Platelets were up from 30 to 34, and neutrophils from 1.09 to 1.41.
Both Dr. Klotz and I were ready to chalk these increases up to sampling error or some effect of drawing the blood through a PICC line. I got ready to sit for two hours of Campath and four hours of RBCs.
But, after Dr. Klotz met with his colleagues and the attending physician, Dr. Tisdale, the plan changed. Visiting my room with the team, Dr. Tisdale noted that a few folks have seen their blood production bounce back more quickly than is the norm after the initial assault from the Campath. That could be the case here, he said, and, given that I'm experiencing no significant distress from low hemoglobin, we might as well wait until tomorrow's CBC to make a decision.
He noted that tomorrow's tests will include a count of reticulocytes -- immature red blood cells that circulate in the peripheral blood for a day before turning into grown-up red cells. We measured 59,000 of those per microliter before the Campath; they were at 23,100 two days ago. If they are back up to pre-Campath levels, we'll have an inkling that my RBC factory is recovering from the onslaught of Campath and we might wait and see what happens.
Another consideration pointing in that direction, according to Dr. Tisdale, is the fact that any transfusion carries with it some risk. So avoiding them, if possible, is always better. To that point, one of the things I've discovered since coming to NIH is that I have picked up a new antibody to complicate blood procurement. I had already developed the anti-e antibody, and now I have anti-C as well. The NIH Transfusion Science department sent an official notification of the same to my home, complete with wallet card to present to my local oncologist's office and blood bank.
I am still going to treat today's uptick in the counts as a sampling error until confirmed by additional data, rather than getting my hopes up. And even if my production is struggling to get back up to its pre-Campath levels, those levels were no great shakes. The median time to response in this trial -- i.e., improvement in any blood line -- has been three months, so there's a ways to go before we know whether the Campath has worked.
But it sure would be nice to walk out of here not expecting to have significantly more frequent transfusions than when I walked in.
Note that they found a stray lymphocyte swimming around in today's sample. I reckon that's why we are doing this for ten days: we got to get 'em all!
 Campath N&L
Campath N&L by
hankins.greg, on Flickr