Lori,
Absolutely every presentation I've watched, every webinar I have reviewed, and everything I have read on full-intensity vs. reduced intensity stem cell transplant has said the same thing: It's a tradeoff between transplant -related mortality and relapse. "Transplant-related mortality" is doctor-speak for "the transplant kills you." (I'm not positive, but I think this would include any reaction to or inability to withstand the drugs or radiation, as well as acute GVHD occurring within a few months of transplant.)
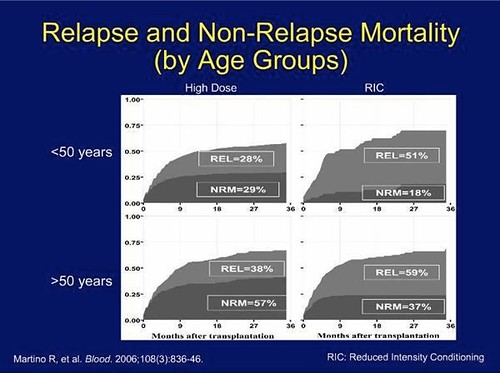
With a full-intensity transplant, the patient is more likely to be killed by the transplant process, but far less likely the relapse. With a reduced intensity transplant, the patient is far less likely to be killed by the transplant but more likely to relapse.
Almost everyone uses the same study -- and even the same graphs -- in their presentation to demonstrate this, from a 2006 European study published in the journal Blood, that pulled together statistics on nearly 850 patients.
I'll try to provide some more details on the findings of that study later today if I can steal a little time from work.
But all this makes me wonder if what your doc was saying is not that the risk of relapse is the same with a full-intensity vs reduced intensity transplant but rather that the overall chance of cure/risk of death work out being the same either way. That's what the 2006 study demonstrated.
Of course, you are an individual, not a statistic, so it's better to understand the statistics and then understand why you have a better than average chance of a successful transplant.
More to come . . . .
Take Care,
Greg
Here are the graphs:
 13.SCT Comparison Study
13.SCT Comparison Study by
hankins.greg, on Flickr
Just looking at the over-50 What the graph says is that, over a three-year period, the chance of "NRM" -- Non-Relapse Mortality -- is 57% with