
| Home Forums |
|
#1
 Fri Oct 7, 2011, 10:08 AM
Fri Oct 7, 2011, 10:08 AM
|
|||
|
|||
|
Talking Telomeres
I've been pretty absent from this space for a couple of months, and I think I know why. As a reporter, I'm more apt to write about my MDS when there's a story to tell. When it appeared that my Campath story had played itself out without a fully successful conclusion, I lost the plot line.
Yesterday, my MDS got its groove back. I had a call from Dr. Bogdan Dumitriu, a fellow at the National Institutes of Health. I met Dr. Dumitriu during my follow-up visits in the Campath trial. He called today to share some very, very interesting news about my MDS. When I signed up for the Campath trial at NIH, I also signed a separate protocol that allows the lab to take extra blood and bone marrow samples, for use in other research. One line of research being pursued by Dr. Neal Young, Dr. Phillip Scheinberg, and others involves telomeres. As I understand this, telomeres are little tails of material on the tip ends of chromosomes. They don't have much genetic significance, but they serve a very important protective function. When a chromosome divides, it's important that it splits at just the right place, so that a chunk of one of the new chromosomes doesn't get torn off and remain attached to the old chromosome. The telomere is where the split happens. [IMG] 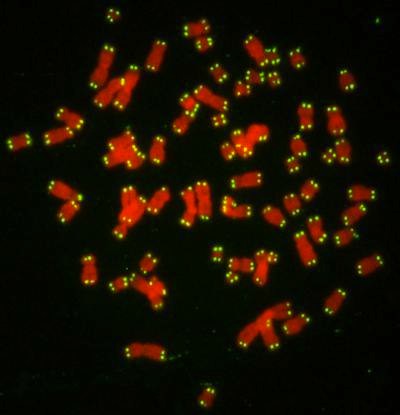 071004143131-large by hankins.greg, on Flickr[/IMG] The telomere is like a bit of sacrificial tissue at the break point that prevents the more important bits of the chromosome from being damaged during division. As we get older, our telomeres get shorter, so they don't work as well to protect the important parts of the chromosome, and we're more likely to suffer chromosomal damage. It's possible that these shorter telomeres may be one of the causes of MDS -- and one of the reasons MDS is so much more common in older folks. It turns out, Dr. Dumitriu tells me, that my telomeres were tested at NIH, and they are very, very short. What counts as "short" varies by age. As a 54-year-old, my telomeres are shorter than 99 percent of all other 54-year-olds. In other words, my age-adjusted telomere length places me in the first percentile of telomere shortness. Every time a cell divides, it loses a bit of telomere. But some of that can be added back on by an enzyme called telomerase, which has a protein component called telomerase reverse transcriptase [TERT] and an RNA component called telomerase RNA component [TERC]. Both TERT and TERC have their respective genes, and, Dr. Dumitriu tells me, I have a mutated TERT. There's not much telomerase in your garden variety human cell. It's only needed where there's a lot cell division going on. The bone marrow would be one place, since the marrow has to crank out billions of new blood cells every day. Another place would be in a tumor. Cancer cells divide so fast that they would literally work their little telomere tails off if they didn't have an ample dose of telomerase helping rebuild those tails. Studies in the lab have shown that male sex hormones -- androgens -- can increase telomerase activity in bone marrow stem cells. Studies in people have shown that folks with TERT mutations and low telomerase activity can regain normal telomerase activity by taking androgens. So, the NIH has developed a clinical trial using mail sex hormones -- in this case, a synthetic testosterone called Danazol -- in folks with aplastic anemia or other bone marrow failure diseases who have tiny telomeres or TERT or TERC mutations. Folks with a lung disease (Idiopathic pulmonary fibrosis) are also included in the trial, because TERT mutations are also implicated in that condition, as well as in liver disease. Danazol was evidently used decades ago to treat folks with Severe Aplastic Anemia with some success. The folks at NIH think that may have been because of this effect on telomeres. They've invited me to come up to NIH for further screening for the Danazol trial, which is described here. Several folks on marrowforums are already enrolled in the trial; they've started talking about their experiences here. So far, they all seem to be aplastic anemia folks with a TERC mutation, instead of MDSers with a TERT mutation. Either way, it will be good to have company if I wind up doing the trial. Reading about telomeres, it seems that there may be at least two ways that they can mess up bone marrow, though this may be more conjecture than established fact, at this point. When a stem cell with a short telomere divides incorrectly, that can trigger the internal functions that cause programmed cell death. Producing lots of defective stem cells and other progenitor cells that die young, after a while, can start to create a shortage of stem cells and cut seriously into the production of good, usable blood cells. This seems to be the problem for folks who have telomere-related AA. The other problem occurs when a short telomere produces a faulty chromosome division that results in a defective stem cell -- and that stem cell doesn't die, but starts reproducing defective copies of itself. Now we have a clonal disorder, like MDS. The next step is to head up to Bethesda for screening -- something that is likely to happen sometime in November.
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com 
|
|
#2
Fri Oct 7, 2011, 10:58 AM
|
|||
|
|||
|
Hi Greg, good to see you back in action... I've been following Dr Ornish since the beginning of the year after seeing show on aging and Ornish talking about being able to increase telomeres via his lifestyle changes. He has a study on his website ( http://www.pmri.org/research.html#telomere-study) and link to this abstract ( http://www.ncbi.nlm.nih.gov/pubmed/18799354 ) and a google search will pull up additional info that you may want to take a look at. I've been following his program since March and I'm still fine tuning the diet portion of it I originally went vegan which he does not advocate but made additional adjustments to move closer to his reversal diet. Anyway I know your research capabilities are far above mine so I hope you turn up some positive thoughts on this.
__________________
Tom- 62 yrs old, dx-eosinophilic fasciitis 2004, 1 yr prednisone resolves EF- now low counts, HGB has been ok... EF has been associated with MDS along with AA.
|
|
#3
Fri Oct 7, 2011, 11:03 AM
|
|||
|
|||
|
That's an excellent explanation, Greg. We've heard Dr. Young report on this line of research and treatment at patient conferences and it sounds more and more promising.
One way we've heard telomeres described is that they are like the tips of shoelaces, called aglets, that keep the rest of your shoelace from unraveling. As long as your aglet lasts it keeps the string of your shoelace from becoming frayed. But if your aglet is lost the ends of the string are exposed and can start to unravel. In the analogy your chromosome is the shoelace. The genes that matter (the string) are protected by the telomere (aglet) on the end, which contains filler. It takes the beating so your important genes don't have to. People with short telomeres are more likely to end up with bad chromosomes after call division. When aglets wear out you replace the shoelace. With telomeres you coax them into growing as they are supposed to do normally. I hope you make it into the trial.
|
|
#4
Fri Oct 7, 2011, 11:05 AM
|
|||
|
|||
|
Hey Tom!
Nice to hear from you. I will definitely check out the links. Do you know you have short telomeres, or are you just working on counteracting the normal age-related shortening? Thanks! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#5
Fri Oct 7, 2011, 12:19 PM
|
|||
|
|||
|
Greg, No I do not know the status of my Telomeres, I got on this path from looking into what to do while in watch and wait mode. I knew and read about his study on telomeres but didn't make much of it as I figured it didn't have anything to do with MDS. I looked into what Bruce and Marla over at aplastic central did but could never really connect all the dots. What they are doing is very close to the ornish program, Bruce recommends macrobiotics and books by Sherry Rogers I could not figure out what the heck is going on with that but she does give a plug for ornish saying that is a good program. When I looked at doing something through diet Ornish kept popping up, so that's how I ended up on the ornish program. My thought process was that I didn't want to stir the hornets nest and this plan seemed like it was well thought out.
I originally was on a vegan tilt to his diet, trying to get the best of his plan and what was in the anti cancer book you suggested and the china study. But I have since added in eggs and no fat dairy, I'm pretty close to the Ornish reversal plan. I misunderstood some information on fruits and fruit juice for the first 5 months and was off the plan by a wide margin in that regard. Fruit on the ornish reversal diet is limited to 4 servings a day and I must have been at about 20 it took a while to sink in why that was bad but when I looked up the impact of fructose on the body it made sense. ( Both Marla and Bruce had posts to that affect but like I said it didn't hit me right away ) this video (http://www.uctv.tv/search-details.aspx?showID=16717) might be worth your time.
__________________
Tom- 62 yrs old, dx-eosinophilic fasciitis 2004, 1 yr prednisone resolves EF- now low counts, HGB has been ok... EF has been associated with MDS along with AA.
|
|
#6
Fri Oct 7, 2011, 12:40 PM
|
|||
|
|||
|
Quote:
That is a way cool analogy -- and an even cooler word. I've been handling those little shoelace tips several times a day every day of my life and I never, ever, knew that they had a name. "Aglet." I like it. I'm going to drop it into casual conversation as often as possible just to watch folks' brows furrow. Thanks much! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#7
Fri Oct 7, 2011, 12:44 PM
|
|||
|
|||
|
Tom,
Thanks again. It seems like telomeres are kind of a hot commodity in the research world these days. I noted in one thing I ready that the folks who sorted out the whole telomerase deal won a Noble Prize in 2009,. so that probably caught a lot of folks' attention. I admire you persistence with diet. I am such a diet slob. Not that I eat a lot of bad stuff, but I'm not very disciplined at sticking to a program. I'm going to check out the Ornish stuff and the links you provided, now that I know for sure I have tiny telomeres. Thanks! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#8
Fri Oct 7, 2011, 02:46 PM
|
|||
|
|||
|
Short telomeres
Hi Greg,
Too bad with your very short telomeres  ! As far as I understand that isn't a positive sign and perhaps you need more active treatment than Danazol. If you are accepted in that trial you could leave it if your counts continue to decrease. ! As far as I understand that isn't a positive sign and perhaps you need more active treatment than Danazol. If you are accepted in that trial you could leave it if your counts continue to decrease. Kind regards Birgitta-A
|
|
#9
Fri Oct 7, 2011, 03:16 PM
|
|||
|
|||
|
Hey Birgitta!
I think you are right. At least, in my reading so far, it appears that AA folks with short telomeres are less likely to respond to immunosuppression, are more likely to relapse after immunosuppression, are more likely to relapse after transplant, and are more likely to have complications during transplant (mainly because of hidden lung and/or liver problems that are also linked t the short telomeres). There seems to be less information on MDS and telomeres, but Dr. Dumitriu tells me their team is confident that TERT and TERC mutant folks are all fighting more or less the same problem, whether it's expressed clinically as MDS or AA. Even though this mutation is not particularly good news, given all those bad odds, I oddly feel more positive and energetic about the fight, now that I have more information about what I'm fighting. What appealed to me about immunosuppression and the Campath trial was that it made sense. It was a narrative, with a plot line that I could understand. By contrast, some of the other options seem more like throwing the pasta against the wall to see if it sticks. I suppose I'm just very story-oriented. So knowing that I have this TERT problem, that it's an active field of research, and that there are things we can try, all that makes me more hopeful and confident. In other words, I'm a little bit crazy. Maybe MDS makes you a little bit crazy after a while. I'm also concerned about my daughters, who will need to be tested for the mutation. But, apparently, plenty of folks with the mutation never have clinical symptoms (and neither smokes, which is very good). My platelets and neutrophils have both been hanging in at the bottom end of normal after rebounding post-Campath. The problem is the increased need for RBC transfusions, and I'm hopeful that the Danazol will address that. But, if it doesn't pan out, or symptoms get worse, I could definitely withdraw from the trial and try something else (assuming I'm accepted in the first place). I hope you are doing well! Take care! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#10
Fri Oct 7, 2011, 03:44 PM
|
|||
|
|||
|
Danazol
Hi Greg
Oddly enough, Danazol is the next step for me....I am going on 200mg/day (100 2xday), probably in the next week. My Drs think is it good going forward, but say it takes a few months to work. I have to postpone more chemo--Dacogen is the next logical step--until this fever issue resolves.....I think its from a low WBC... What is the dosage at the clinical trial? And what is the advantage to doing a clinical trial, rather than have your Dr prescribe it for you? Since I live alone, Clinical trials are virtually impossible. All I know is that I have 0 energy and something has got to give!!!!
__________________
Cheri Age 54; dx Oct 2009 AML, induction chemo only;dx MDS July 2010,- PRBC transfusion dependent; Results BMB 8/4/11--- 6-8% blasts; Danazol 100 mg 3xday; quit Exjade/ GI distress; platelets holding 40's; Fluctuation in blasts in blood--Neupogen 3-4xweek; off Revlimid again! Procrit weekly
|
|
#11
Fri Oct 7, 2011, 03:53 PM
|
|||
|
|||
|
Danazol
Hi Greg,
Good that you feel more confident  ! We hope that you will be accepted and that Danazol will improve your HGB. ! We hope that you will be accepted and that Danazol will improve your HGB. I am still OK after 16 months with Thalidomide and Prednisone. Latest counts: HGB 13.5, WBCs 4.4 and platelets 92. Kind regards Birgitta-A
|
|
#12
Fri Oct 7, 2011, 05:00 PM
|
|||
|
|||
|
Quote:
I've been reading about your struggle with this fever; I hope it gets under control soon. Dr. Dumitriu tells me the dose is 400mg 2x/day -- so 800 mg per day, which is pretty huge! The dose can be halved if necessary, though they figure that will be rare. For me, the clinical trial participation sort of feeds into my whole desire to have a storyline, know what the theory is behind using the drug, and so on. Plus, I figure that whatever they learn from me will help someone else down the line. From a practical perspective, the drugs and treatment at NIH are free, since it's a government operation. That definitely beats negotiating with my insurance company to try to get them to cover an off-label use (though I haven't really tried that, so I don't know how much of a problem it would be -- probably not much with an old drug like Danazol. I haven't checked the price, but surely it's not too expensive. Getting them to pay for Revlimid, on the other hand, might be a lot harder, if I went that route.) My wife generally goes with me when I travel to Bethesda, though I suppose I could swing it on my own. I did have that one fainting spell after a bone marrow biopsy . . . that wouldn't have been too fun on my own. If that gator gets too close, give him a kick for me! Take care! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#13
Sat Oct 8, 2011, 01:09 PM
|
|||
|
|||
|
dear Greg,
your telomere- and telomerase-story is sth. very new for me. Although I have known the correlation of age and the length of telomeres. I once read, that to solve the problem of telomeres becoming shorter by age, it could mean to make immortality possible (mankind's dream, not a good idea) How did it occur to your docs to examine your telomeres? And how did they find your special mutation? Is this part of the normal cytogenetic analysis? I am very curious to get to know about the effectiveness of Danozol in this case. Testosteron, mhh, does this fit also for women?  I support your positive sight - in fact I am too pessimistic from time to time - keep us informed, Bergit
__________________
female, 54, MDS-RCMD, trisomy 8, dx 2006, response to EPO and therafter VPA only for a couple of months, transfusion-dependent twice a month, watch&wait for SCT somewhen in the future with my brother as a donor 
|
|
#14
Sat Oct 8, 2011, 03:26 PM
|
|||
|
|||
|
Hi Bergit!
When I consented to the Campath trial, I consented to also have additional vials of blood drawn "for research purposes" on each of my visits to NIH. At the time I signed the consent, I asked the research nurse what sort of studies my blood might be used for, and she mentioned work they were doing on telomeres. So I think these extra vials were the reason I was tested; testing for either telomere length or TERT & TERC mutations is definitely not yet part of of the standard diagnostic toolkit for MDS in the US. I gather that measuring telomere length is pretty difficult and expensive. But there is a commercially available test for the mutations. I'll bet that, in five years of so, it will be common to have a battery of genetic tests for folks with MDS. Dr. Neal Young, Dr. Rodrigo Calado, and Dr. Phillip Scheinberg, all at NIH, have published quite a few papers over the past decade on telomere length and TERT & TERC mutations and their association with bone marrow failure -- particularly Aplastic Anemia. This appears to be a very active area of research that is only now coming out of the lab into the clinic. One of their studies that examined AML patients found TERT mutations associated with Trisomy 8, but I haven't found any follow-up on that as of yet. Interesting point about female use of Danazol: the first use for the drug in the US was as a treatment for endometriosis -- in the early 1970s. But it can result in unwanted hair growth, apparently. I think it has also been used for doping by athletes. Though I don't completely understand the mechanics of this, I've read that excess testosterone is "aromatized" into estrogen analogues in the human body, so that male bodybuilders using synthetic testosterone can find their breasts enlarging. But, thankfully, I have read nothing about this as a possibility in the list of Danazol side effects (though those lists seen to focus on use of the drug by women). I will definitely be posting an account of my experience in the trial here and on my blog, if I'm accepted. And other marrowforums folks -- all ladies, so far -- are also on the Danazol trial. I hope you are doing well; it's nice to hear from you. Take care! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#15
Sat Oct 8, 2011, 03:35 PM
|
|||
|
|||
|
Telomere articles
Hi All!
I've been reading up on telomeres, TERT & TERC mutations, and bone marrow failure. I've found a couple of review articles that are available free in full text. Those of you who are, like me, inclined to occasionally torture yourself by trying to understand stuff that's way above your pay grade might find these interesting. Telomere maintenance and human bone marrow failure, by Dr. Calado & Dr. Young of NIH Telomeres and Marrow Failure, by Dr. Calado (This one is a PDF file.) Have fun! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#16
Sun Oct 9, 2011, 11:14 PM
|
|||
|
|||
|
Comments on Danazol:
I've been on it for two or three years. It took several months for me to notice any effect. I have been able to reduce my cylosporine since I took it. Cyclosporine is hard on kidneys, but Danazol is hard on the liver. It has the side effect of making red blood cells. That is why I take it. It is also why it is a banned substance for the Olympics. I no longer can have my Olympic dream, but I may be able to ride in the Tour de France. I notice a slight increase in confidence and people who bother me since I've taken it. Yes, I have "man boobs". But I already had them from the the large doses of prednisone and cyclosporine I took in the past. I'm sure my female hematologist here in Dallas secretly felt for breast cancer one time. If these can slow the aging process, I'm hoping for the Benjamin Button effect to start kicking in. Just be thankful that places like NIH have the interest and funds to study these things. All of this science may apply to more than just the areas we are familiar with.
__________________
Dallas, Texas - Age 81 - Pure Red Cell Aplasia began March 2005 - Tried IVIG - Then cyclosporine and prednisone. Then Danazol, was added. Then only Danazol . HG reached 16.3 March 2015. Taken off all meds. Facebook PRCA group https://www.facebook.com/groups/PureRedCellAplasia/
|
|
#17
Wed Oct 12, 2011, 12:40 AM
|
|||
|
|||
|
Wow, Greg, you keep the plot twists coming to the mystery that is this disease...I'm soooo glad you got into the NIH system. Another bad news, good news story - short telomeres (ugh), but how would you have known without the Campath trial...and, while I didn't know about the reporter background, we all agree you are a gifted writer.
__________________
Catherine, wife of Bruce age 75; diagnosed 6/10/11 with macrocytic anemia, neutropenia and mild thrombocytopenia; BMB suggesting emerging MDS. Copper deficient. Currently receiving procrit and neuopogen injections weekly, B12 dermal cream and injections, Transfusions ~ 5 weeks.
|
|
#18
Thu Oct 13, 2011, 12:09 AM
|
|||
|
|||
|
Hey Catherine!
Yep, I'm beginning to think that the NIH and I were made for each other: we both have way too many questions. And I've discovered a new term for the "story-based" treatments and trials that I find most appealing: "rationally-designed." Evidently, that's code for "We saw something interesting, we developed some hypotheses, we did a bunch of tests in the lab, we came up with some more questions, more lab work suggested this might be a treatment angle, so now we're going to check that out with a clinical trial." The other way of doing business is more like: "We've got this great drug that's working for multiple myeloma . . . let's try it on some MDS patients!" Those are both caricatures, of course. There are plenty of really smart folks out there in the pharmaceutical companies looking for new uses for their drugs. And, in the end, if a drug works, it works. But I do have a weakness for the "rationally-designed" approach. It does seem like it's all good news-bad news in this bone marrow failure business. But my experience just shows how important it is to keep looking for answers and working with a variety of docs. My local hematologist told me he would never have thought to check for a copper deficiency; it was only my university-based transplant consult who came up with that angle. And my local doc (and the transplant doc) was highly skeptical of immunosuppressant therapy, until I gave him one of Dr. Sloand's last articles and my HLA profile from my university doc. Now, none of that has panned out as I had hoped, but it all made sense. And this short telomere thing makes sense. As Dr. Olnes told me in an email this morning, MDSers with tiny telomeres are prone to relapse, and that may explain why my reticulocytes bounced back so strongly immediately after Campath, and then fizzled. I'm still waiting to hear from the research nurse at NIH to set up a screening appointment for the Danazol trial, but the more I read about telomeres, the more it makes sense to give this a shot. I'm still not clear on exactly how common short telomeres are amongst MDSers; I'm probably going to be driving some NIH docs nuts with questions. Hope you and Bruce are doing well. Got plenty of firewood laid away for the winter? Take care! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#19
Fri Oct 14, 2011, 04:25 AM
|
|||
|
|||
|
Hi, Greg...lots of wood! Bruce has about 2 cords stacked so far. He is waiting to bring down more, but I'm still watering (darn it), and it's getting in the way of his stacking.
We were in Portland yesterday for Bruce's bone marrow biopsy, and the hematologist we consulted with last year popped in. It was very nice of him to do that, we didn't have an appointment with him. But since he was there, I talked telomeres a little bit with him, casually mentioned TERC and TERT -- he said "everybody's telomeres get shorter as they age." But then said they would do some extra genetic testing...so we'll see what they come up with. The PA who does the bmb's later said that we had caught him up short with the question about telomere's, so I gather this is very much cutting edge stuff. I really wasn't trying to seem snobby, lol, I've just learned so much here. We did make an appointment to go see Dr. Paquette again at UCLA, gosh we're getting a long list of questions for him. Meantime, the good news is that Bruce's hgb and hct haven't dropped so drastically since the last transfusion. The bone marrow biopsy is the big waiting game, of course. I'm glad you are well positioned to take advantage of the trial, if you decide it's the direction you want to go. The drug's antecedents are interesting. Hugs, Catherine
__________________
Catherine, wife of Bruce age 75; diagnosed 6/10/11 with macrocytic anemia, neutropenia and mild thrombocytopenia; BMB suggesting emerging MDS. Copper deficient. Currently receiving procrit and neuopogen injections weekly, B12 dermal cream and injections, Transfusions ~ 5 weeks.
|
|
#20
Sun Oct 16, 2011, 09:40 AM
|
|||
|
|||
|
I haven't visited the forum in quite a while. While I am doing well, I guess I like to stay away from it, but I was wondering how you were doing since I last read that Campath was not successful for you.
Yes, NIH sure does take their research samples, but VERY positive that they called you to consider the telemere trial. I would go for it, if it was me. My last bmb down there was extremely painful; I hope the next doc is better at it! I wish you great luck and keep us posted if you end up doing it. So disappointed that Dr. Olnes has moved on, but I am looking forward to meeting Dr. Scheinberg on my visit in March for my 3 yr follow up. I will keep you in my thoughts and prayers! Keep fighting!
__________________
Dx. 6/08 with AA, then changed shortly thereafter to MDS. Campath trial at NIH March '09 and have been transfussion independent since June '09
|
|
#21
Sun Oct 16, 2011, 09:46 AM
|
|||
|
|||
|
one more thing to all!
I forgot to mention that thanks to the Campath trial I did 2.5 years ago at the NIH, I am now going to get the experience of being a 1st time GRANDMA! While the "circumstances" are not ideal, (this wasn't planned; my son lives at home, his girlfrield splits her time between her house and here; both have low paying jobs; both are in early 20's), this is the reality of it all. It is kind of bitter-sweet for me. BUT the baby will be here in 5 1/2 weeks and I know I will be thrilled. It just makes me so nervous with them having a baby at this point with the lousy economy and I just hope I am around a long time to lend a hand.
__________________
Dx. 6/08 with AA, then changed shortly thereafter to MDS. Campath trial at NIH March '09 and have been transfussion independent since June '09
|
|
#22
Sun Oct 16, 2011, 02:16 PM
|
|||
|
|||
|
Babies are the best, no matter the background circumstances. You will not believe the life force the baby will provide you and everyone around it. You are truly lucky!
Donna
__________________
f68 MDS; abmt 1/12. ABO mismatch 11 mos. (70) transf. Ferr 3-5k. 8 phlebot. AGVHD to CGVHD. skin,eyes. lungs as of 10/13. muscle weakness &osteo long term steroids.photopheresis 2x wk as of 3-15.pred 20 eod,acyclovir, mepron, voriconazole, pantropazole, lisinopril, montelukast, anoro, azithromycin.
|
|
#23
Sun Oct 16, 2011, 06:10 PM
|
|||
|
|||
|
ok. these telomeres are very interesting, from what I can unerstand of it...my spouse is having a BM next week. Would it be a good thing to get her to have the test included as well? Also will ask her about the tellomeres and MDS.
He is starting his 6th set of Vidaza this week as well, and the counts seem to be holding. We had a 7 day vacation in the Turks last week, he even snorkeled every day, the breathing was fine...he had such a smile. Thanks to all who have gone before with the drug trials.
|
|
#24
Fri Oct 21, 2011, 12:39 PM
|
|||
|
|||
|
Quote:
Sorry for the slow response. I was in Nashville working 12-hour-plus days rehabbing the bathroom in my daughter's new old house. Came back, four weeks after my last RBC transfusion, to find my HGB at 6.3. So I'm now having three units. Glad you have lots of wood stacked. I just read there's a good chance we'll have a mild winter, which would be just fine with me. The telomere story is pretty fascinating stuff. Turns out there are three ways of measuring them, one of which has my favorite name so far for a lab procedure: "Southern blot." This sounds like it should be a version of the Rorschach test for folks who live south of the Mason-Dixon line -- or maybe what you feel like after consuming half a fifth of Jack Daniels. I didn't get the Southern Blot, however. Nor did I get the Flow-FISH, which records telomere length in each of a half-dozen different types of white blood cells (leukocytes). Instead I got the quantitative polymerase chain reaction (qPCR), which just gives one number based on all types of WBCs. I asked for a copy of the report and got a single page with this scatter chart in the middle of it. [IMG] 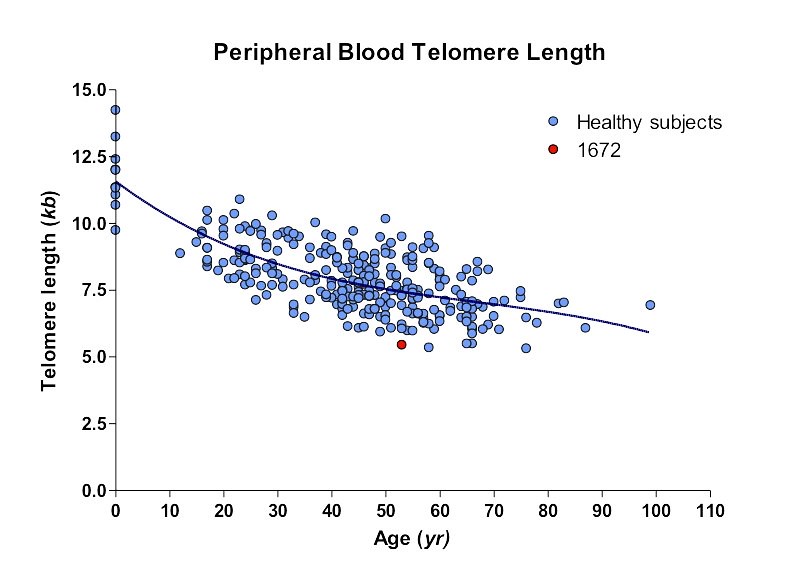 Telomeres3 by hankins.greg, on Flickr[/IMG] The little red dot is me. If you look at the graph a while, and notice the trend line, you can see that I have a telomere length that would be short for the average centenarian (though the sample out there in the big numbers is pretty small. There's also a big spread in the sample of healthy subjects. But I'm 2.3 standard deviations below the age-matched mean. I'm not really sure how much the test costs, but there's a lab up in BC that offers it commercially, so Bruce's doctor should be able to order the test if you want to check it out. Take Care! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
|
#25
Fri Oct 21, 2011, 12:51 PM
|
|||
|
|||
|
Quote:
Congratulations on the grandbaby! It's great to hear from you -- and I'm glad the IST is still working for you. Donna J is right: babies can be transformative experiences, particularly if the young couple has a good support network. Marcy and I were married and had our first child as Juniors in high school. We're still together 37 years later. Both daughters are happy, healthy, and pursuing their dreams in the arts. None of us is wealthy, but we are all happy, and we all still support each other. Good luck! Greg
__________________
Greg, 59, dx MDS RCMD Int-1 03/10, 8+ & Dup1(q21q31). NIH Campath 11/2010. Non-responder. Tiny telomeres. TERT mutation. Danazol at NIH 12/11. TX independent 7/12. Pancreatitis 4/15. 15% blasts 4/16. DX RAEB-2. Beginning Vidaza to prep for MUD STC. Check out my blog at www.greghankins.com
|
 |
| Thread Tools | Search this Thread |
|
|
 Similar Threads
Similar Threads
|
||||
| Thread | Thread Starter | Forum | Replies | Last Post |
| Short Telomeres and MAA | KatailS | AA | 1 | Mon Mar 20, 2017 10:35 AM |
| Gene Identified for Short Telomeres in association with Aplastic Anemia | curlygirl | AA | 8 | Wed Oct 1, 2014 09:25 PM |
| The first telomerase inhibitor in trials | Birgitta-A | Drugs and Drug Treatments | 12 | Wed Jan 18, 2012 12:47 PM |







